Hernia surgery is one of the most common surgical procedures in the United States — over 1 million inguinal hernia repairs are done each year. Most patients recover smoothly. But a significant minority experience pain that lingers for months, and understanding when this is normal versus when it signals a problem makes all the difference.
Is It Normal to Have Pain Months After Hernia Surgery?
The answer depends on how many months and how severe. Here is the breakdown:
| Timeframe | Pain status | Action needed |
|---|---|---|
| Weeks 1–3 | Significant pain — normal | Follow standard recovery protocol |
| Weeks 3–6 | Mild–moderate pain — normal | Monitor, follow up at 6-week appointment |
| Months 2–3 | Mild discomfort — borderline normal | Mention to surgeon at follow-up |
| Beyond 3 months | Any significant pain — not normal | Request evaluation and imaging |
| Worsening at any point | Abnormal — red flag | Call surgeon promptly |
What the research says about long-term hernia pain
Studies consistently show that approximately 10–12% of patients develop chronic post-herniorrhaphy pain (CPHP) — defined as pain persisting beyond 3 months after hernia repair. Of these, about 2–4% have pain severe enough to affect daily activities. The remaining 6–8% have mild, intermittent discomfort that gradually improves over 6–12 months.
Which type of hernia repair causes more long-term pain?
Open repair (Lichtenstein technique) has a slightly higher rate of chronic pain — approximately 12–15% — compared to laparoscopic repair (TEP or TAPP) at approximately 6–10%. This is largely because open repair involves more direct handling of the inguinal nerves. Laparoscopic repair, when performed by an experienced surgeon, results in less nerve trauma and lower rates of chronic pain.
What Causes Pain After Hernia Surgery That Won't Go Away?
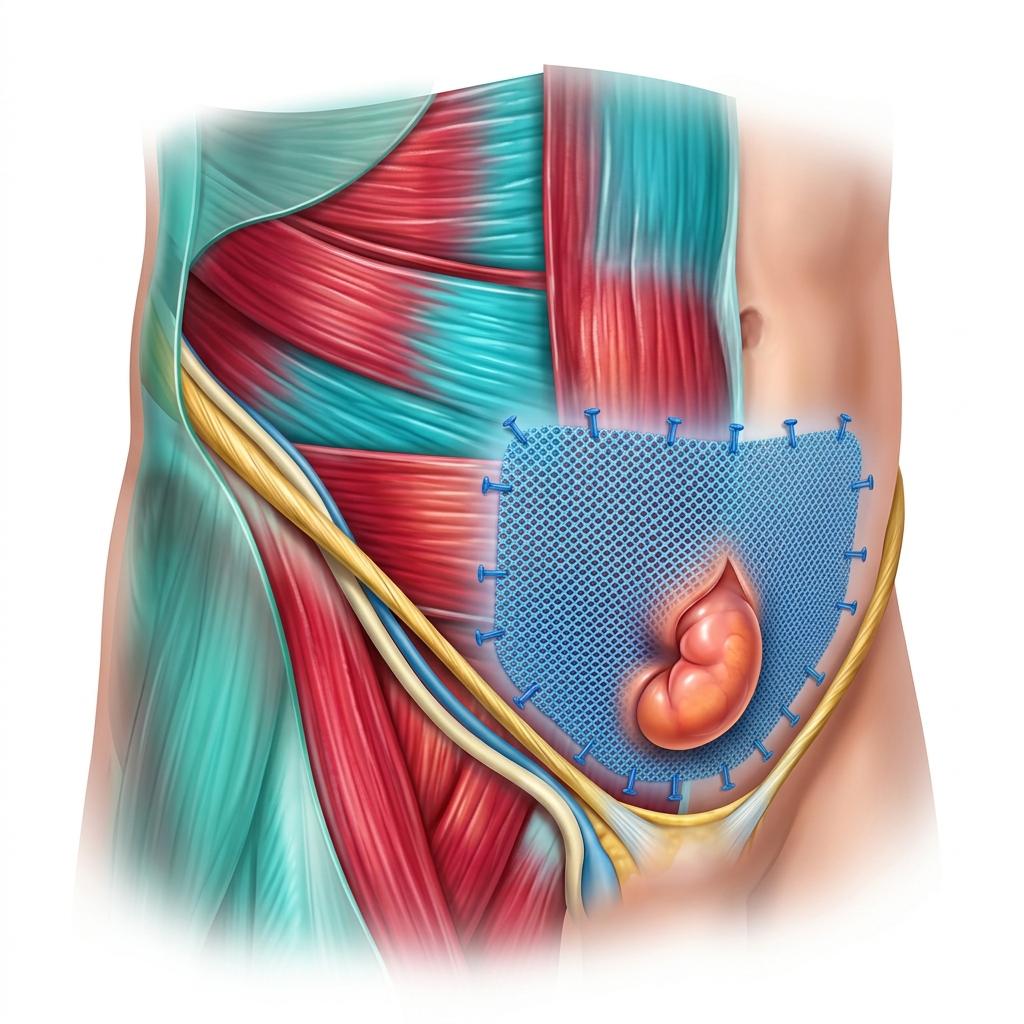
Mesh-related complications
In some patients, mesh triggers an excessive inflammatory response or contracts as it integrates with surrounding tissue. This can cause a chronic aching, pulling, or burning sensation in the groin. Mesh-related pain typically develops 4–8 weeks after surgery — later than immediate post-surgical pain — and has a constant rather than intermittent quality.
Nerve entrapment
The most common cause of chronic pain after hernia surgery is entrapment of one or more of the three inguinal nerves in sutures, mesh, or scar tissue. The pain is typically sharp, burning, or shooting, and follows a specific nerve distribution — down the inner thigh, into the scrotum or labia, or across the lower abdomen. A nerve block injection that temporarily eliminates the pain confirms nerve entrapment as the cause.
Scar tissue and adhesions
In some patients, scar tissue restricts movement of the hip flexors or surrounding muscles, causing a pulling or tightening sensation with specific movements — particularly hip extension, walking upstairs, or rising from a seated position.
Hernia recurrence
Pain months after hernia surgery can occasionally signal a recurrence — the hernia has returned. The telltale sign is a new visible or palpable bulge at the hernia site, particularly with coughing or straining. Recurrence is diagnosed by physical examination or ultrasound.
Treatment for Persistent Pain After Hernia Surgery
Medication options
- Gabapentin or pregabalin — first-line for nerve-related chronic pain
- NSAIDs — for mesh-related inflammation; most effective in months 2–4
- Duloxetine (Cymbalta) — for chronic neuropathic pain beyond 3 months
- Topical diclofenac gel — applied directly to the groin for localized relief
Nerve block injections
An ilioinguinal or iliohypogastric nerve block — injected under ultrasound guidance — is both diagnostic and therapeutic. If it eliminates pain for several hours, it confirms nerve entrapment as the cause. Repeated injections can provide relief lasting weeks to months. Most pain specialists recommend 2–3 injections before considering surgical options.
Revision surgery — when is it needed?
Revision surgery is considered for patients with confirmed nerve entrapment or mesh complications who have not responded to 6+ months of conservative treatment. Options include surgical neurectomy (nerve removal), mesh removal, or mesh revision. Success rates for neurectomy are 70–85%.
Pain Timeline After Hernia Surgery
- A new bulge at the hernia site — possible recurrence
- Fever above 101°F with redness or warmth — possible infection
- Pain that is worsening rather than improving at any timepoint
- Severe pain with nausea and inability to pass gas — possible bowel obstruction (emergency)
FAQ: Pain Months After Hernia Surgery
